Cancer cells express two type of antigens relevant for immune system: major and minor antigens. Major antigens are MHC class I, II and related antigens (HLA in humans). All other antigens are classified as minor antigens. Essentially, when scientists talk about cancer associated antigens they mean minor antigens.
In general, we are tolerant towards both our own major and minor antigens both at B cell or T cell level. This is why it is very difficult for the immune system to spot cancerous cells. Cancer cells must accumulate sufficient number of non-synonymous mutations in its minor antigens before body's immune system can sense it.
New paper in journal Nature discusses new way how to accelerate anti-cancer immunity using allogeneic priming. This is how it works.
The authors employed concept of allogeneic priming. Basically, there are B6 mouse strains which differ only in minor antigens but have the same MHC molecules (antigenic differences between humans are frequently located in minor antigens too).
Depending on number of minor antigenic differences between these MHC-matched allogeneic hosts, immune system of each sub-strain lacks tolerance towards other's minor antigens. For example, B16 melanoma cells are MHC-matched but minor antigenic mismatched in 129S1 substrain of B6 mice and vice versa LMP cancer cells are MHC-matched but minor antigen mismatched in C57 substrain of B6 black mice. Accordingly, each tumor is rejected easily by MHC-matched allogeneic hosts via T cell dependent manner [because of abundance of minor antigenic difference].

Unexpectedly, this rejection was dependent of host B cells too.

Next the authors showed that syngeneic hosts injected with syngeneic BmDCs that were pre-incubated with tumor lysate coated with allogeneic IgG (but not IgM) were protected against syngeneic tumors. (syngeneic cells should have identical major and minor antigens)
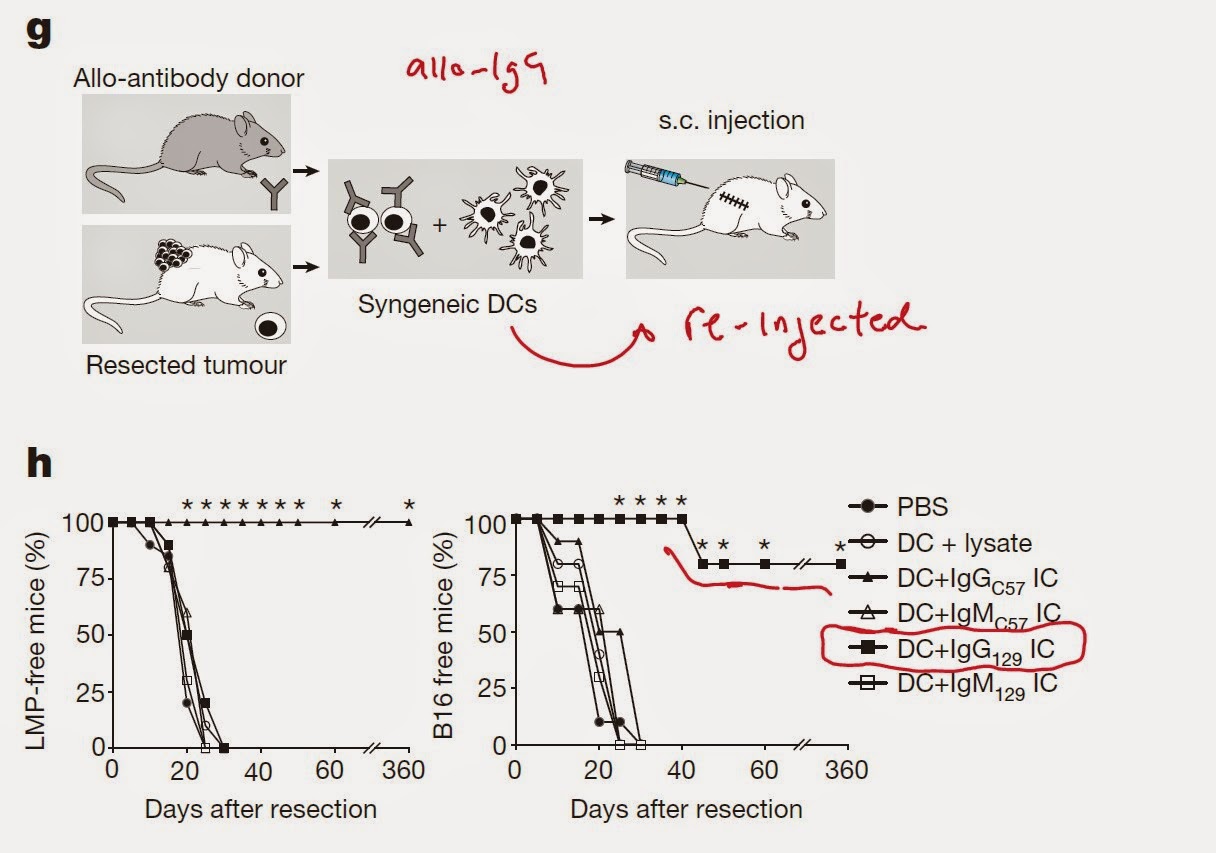
Interestingly, tumor associated DCs (TADC) were incapable of providing such protection, nor direct intra-tumoral allo-IgG injection was effective (however, in Fig. 1k, the authors showed that injection of allo-IgG was effective. Don't know what is the difference).

However, priming with allo-IgG in combination with CD40L/TNF-alpha or PolyI:C could provide anti-cancer immunity. In addition, injection of TADC harvested from immunogenic cocktail treated mice could protect naive mouse against cancer.

In summary, these results (and there are lot of figures) suggest that using allo-IgG priming strategy could help overcome host tolerance towards syngeneic tumors.
How this could apply for human case: one can harvest patient's DCs and incubate with tumor cells coated with allo-IgG. After re-injection, these DCs should then activate patient's T cells and participate in tumor protection.
I don't see that direct injection of allo-IgG in combination with CD40L/TNF-alpha or PolyI:C is a feasible approach though.
Strange thing about this study is the fact that pre-absorbing of allo-IgG serum with normal mouse tissue syngeneic to tumor could abolish protection. If immune system detects normal self-antigens and then initiate cancer immunity, how is then autoimmunity prevented? Most likely, self-antigens are somehow linked to mutant antigens in cancer cells and help to deliver them to DCs for presentation to cancer-specific T cells. Since majority of self-specific T cells are tolerant to self-antigens to begin with, it is less likely that this procedure would initiate autoimmunity.
David Usharauli
No comments:
Post a Comment